Brexit and pharmaceuticals – separating fear from reality
26 September 2018
SUGGESTED

Policies
26 September 2018

Brexit
27 September 2018

Healthcare
4 July 2024
An interview by Sir Michael Rawlins, Chair of the UK medicines regulator the MHRA, sparked concerns that supplies of medicines to patients in the UK would be at risk if no withdrawal agreement is reached with the EU. Sir Michael highlighted the example of insulin, a vitally important drug for people with diabetes, which is not manufactured in the UK. He rightly noted that “the Department for Exiting the EU and the Department of Health and Social Care (DHSC) needs to work out how it’s going to work”.
The Fear and the Reality
What are the reasons behind the fears that supplies of medicines and medical devices will be at risk? Broadly they break down into three categories:
1. Tariffs
Most finished medicines are tariff free under the EU’s Common External Tariff, while most developed countries keep medicines tariff free under a WTO Pharmaceutical Tariff Elimination Agreement. Yet there are some products like active pharmaceutical ingredients and intermediates that are not tariff free and would attract import duties. Most medical devices are also tariff free under the CET. It has been suggested that the UK should work in the WTO to update and extend the coverage of the Pharmaceuticals Agreement.
However, outside of the customs union, and with control over our external tariffs, the UK should unilaterally eliminate all tariffs on medicines and medical devices. Such tariffs are acknowledged to serve no protective purpose in domestic industry, and in this country are largely borne by the NHS. We cannot compel the EU to do the same, so if no free trade deal or transitional period is agreed they may need to apply tariffs to their imports of pharmaceutical products from the UK. While in some cases, depending on whether there is competition for the product, the manufacturer may absorb these, in other cases they will have to be ultimately borne by the EU consumer.
Elimination of tariffs would also avoid the administrative burden of applying for reliefs from duties where ingredients cross borders at different stages of manufacture. As it would take effect a “most favoured nation” basis on all imports from the EU and the rest of world this would also improve competition in the market and value for UK consumers.
2. Regulatory
Because of the sensitive and potentially risky nature of medicines and medical devices, they are subject to rigorous and comprehensive licensing regimes and regulation which is harmonised for the EEA. The EMA is the EU competent authority. The regulatory structure applies both to the products themselves, and to operators in the supply chain, from the holder of the marketing authorisation for the product (MAH) to the manufacturers, importers and distributors (who may all be the same person).
Product approval – marketing authorisation
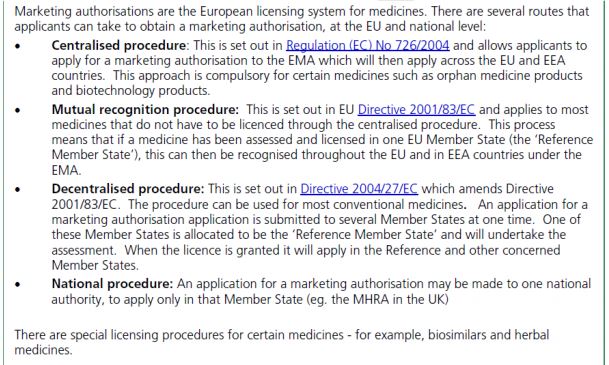
There are different procedures available to achieve a marketing authorisation (MA). A House of Commons Library Briefing Paper summarises them as follows:

It is clear that the different routes mean there are gaps in single market, illustrated by the recent reports of northern European visitors to Spain suffering devastating side effects from taking a painkiller that is widely prescribed in Spain but not authorised on UK market. It is also notable that this has not caused border checks to be carried out between member states, despite such highly material differences – the supply chains are so highly regulated that border checks are not necessary.
Manufacturer/importer licence – MIA
Firms that wish to manufacture or import from a third country medicines that have a marketing authorisation require a licence known as an MIA. For manufacturers and importers in the UK that licence is issued by the MHRA. To qualify for a manufacturers’ licence the holder must comply with certain conditions, which include Good Manufacturing Practice (GMP), a set of principles set out in EU directives. Before issuing a licence permitting import from a third country, the MHRA will need to inspect the manufacturer’s premises in that country to ensure that it conforms to GMP. Each batch of medicine imported from duly authorised third country manufacturers must then be inspected and certified by the Qualified Person (QP) of the licensed importer, unless the manufacturer is in a country with which the EU has a mutual recognition agreement in place in respect of GMP. The EU has such agreements with Australia, Canada, Israel, Japan, New Zealand, Switzerland and the United States. Medicines manufactured in or imported to any EEA country can be distributed in any other EEA country where the marketing authorisation applies.
After Brexit, the UK and EEA members will be third countries to each other. This means that, unless arrangements are made, marketing authorisations issued by the MHRA will no longer be valid in the EEA, EEA importers will need importer licences be permitted to import products from UK manufacturers, and the EEA importers will need to carry out full batch testing on imported medicines from the UK (and vice versa).
Optimally, the EU and the UK will agree to continue to recognise MAs and MIAs issued by each others’ authorities, at least for as long as the UK elects to retain single market regulation in this field. It is intended that this will be the case if the withdrawal agreement is agreed, because the UK’s full participation in the single market will continue for the transitional period.
If the withdrawal agreement is not agreed, or if no final agreement on regulatory recognition is reached at the end of the transition period, fears have been raised that supplies of medicines will be at risk due to these regulatory barriers.
This would indeed be the case if neither side, took any action. While the European Commission and EMA’s notices and actions so far have been oriented at no deal preparedness (for example indicating that MAHs will need to make changes to their MAs, by transferring or varying them to be in the name of an EEA entity by the end of March 2019), it is clearly in the interests of both parties, and especially users of these essential products in the UK and the EU, to reach an agreement that will enable the lowest friction possible in trade in medicines.
If no agreement is reached, there are wide ranging actions available to the UK unilaterally to keep our market open to medicines from the EEA. For example, the MHRA could be empowered to unilaterally recognise MAs issued in the EEA under the central and decentralised procedures, and recognise GMP, GDP and QPs in EEA, to enable imports of medicines manufactured and licensed in the EEA, whilst continuing the MAs that firms already have in the UK. This would need to be conditional on EEA MAHs providing reporting and data to the MHRA that the MHRA would no longer be entitled to from EU databases.
The MHRA has stated that “if no transition period is agreed, we would ensure the minimum disruption and burden on companies as the UK exits the EU, while building on the existing relationship between MHRA and firms.” However its latest publication on 6 August 2018 addresses how the transition period would be implemented and does not provide any proposals on no deal planning. Given the publicity that stories of shortages and stockpiling are attracting, it would be beneficial for the MHRA to publish some information on the steps it can take to avert these scenarios.
Medical devices
Medical devices (which include everything from bandages and syringes to apps) are not subject to the same process of authorisation and licensing. They must meet applicable regulation on safety and be independently certified by a notified body. It is common in international trade to have mutual recognition of conformity assessment, but if this cannot be agreed with the EU the notified bodies must be EEA entities. To secure continued supply of medical devices from the EEA if no deal is agreed, the UK can continue to recognise EEA notified bodies unilaterally. For exports, most UK notified bodies are part of wider European groups, so can continue to certify medical devices for the EEA market as agents or sub-contractors and those that aren’t, like BSi have established a presence in Europe in order to be able to continue to certify products for that market.
3. Logistical delays
While the above unilateral steps would smooth the regulatory aspects, a key concern has been that pharmaceutical supplies will be caught up in delays at ports and airports. To avert this, pharmaceuticals companies and their intermediaries should be prioritised to become certified as Authorised Economic Operators (and for other trade facilitations that are available enabling goods to be cleared without inspection, and payment of duties and VTA to be deferred). Existing supply chain security from rigorous licensing requirements should mean that they will qualify straightforwardly.
The government should also seek recognition of the UK’s AEO scheme from the EU and other trade partners. However, the processes to streamline customs declarations and clearance that HMRC will need to put in place need to be clarified and publicised as a matter of urgency so manufacturers, distributors and their logistics suppliers can make the necessary arrangements. These should include postponed accounting for import VAT, and periodic self-assessment for customs declarations so that not every shipment will need to be declared.
For more details on unilateral facilitation measures that the UK government should be implementing see our briefing Under Control: What HMRC can do to prepare and optimise customs processes for all outcomes. The government is also working with manufacturers and distributors to ensure that sufficient stocks are available in the UK to cover supplies in the event of disruptions from a no deal scenario. The chief executive of the European Association of Euro-Pharmaceutical Companies (EAEPC) has said “excess warehousing provision is being sought by manufacturers in advance of next March so there’s sufficient supply already in place” but this can only be a short term, interim measure.
More strategic/long term concerns
Another important feature of the single market in medicines is the information sharing between regulators – “pharmacovigilance”. This enables data on medicines in the market (like adverse reactions) to be monitored and collated across a large population across all EEA member states. It would be highly beneficial to both sides for such information sharing and cooperation to continue, and there is precedent for this in the case of the agreements between the EMA and its counterpart in Switzerland. Even in the absence of international regulator information sharing, the UK could ensure that MAHs and importers continue to report to them on intelligence and developments from the market as condition for continued recognition of their authorisations.
Achieving MA for a medicine is a costly and time consuming process. The larger the market covered by an MA, the more viable it is to pursue. In the mid to long term this will be a key consideration for UK lawmakers, as there are clear benefits to maintaining alignment if full mutual recognition is available. Such benefits will need to be set against the gains that could be made from improving the regulatory system to encourage innovation and competition. If the UK were to continue to recognise EEA MAs, whilst also making improvements to our national system and working with regulators in other jurisdictions like China, Japan and Australia, to speed up authorisations, as suggested by Sir Michael Rawlins in his evidence to the HOC Health and Social Care Committee, this could mean the UK will benefit from more medicines being available more quickly.
Clinical trials regulation is acknowledged to be problematic, and the original EU clinical trial directive has been replaced by a new regulation, which will come fully into force in 2020.
The European Federation of Pharmaceutical Industries and Associations reports that 1,500 clinical trials are currently underway where the UK is the sponsor. While this does not affect the imminent concerns around supplies of medicines, the future of those trials, and the operation of clinical trials under the new regulation, which provides for trials to be regulated by a centralised portal, need to be resolved. Ultimately this is an area where the UK can play role in global fora, for example the OECD, which is calling on “member governments to harmonise their clinical trial approval processes. The aim is to encourage international collaboration in clinical research and streamline procedures for conducting clinical trials”.
Medicines and medical devices regulation is heavily influenced by international organisations like the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). The UK needs to apply for observer status in the ICH as soon as legally possible (ie the first day after we are no longer a member of the EU) in order to progress to full membership after two years under the rules of the organisation. Many people in the industry have suggested the UK having an independent voice in the ICH will be a benefit of Brexit.
For medical devices – participation in International Medical Device Regulators Forum – organisation of regulators from 9 countries (including Japan, the USA and China) and the EU working towards harmonisation and convergence in medical devices regulation.
In any event, investment in the UK by the pharmaceutical sector has remained strong, with Novo Nordisk, Astra Zeneca and GSK all proceeding with significant investments.
The European Perspective
It is becoming increasingly clear that the hard line taken by the European Commission and the EMA is in fact risking the supplies of medicines to the European market. The EMA has announced that due to its move from London to Amsterdam it expects to lose at least 30% of its staff. This, combined with losing the capacity of the MHRA, means that it will be scaling back activities. It is unclear how the additional work it has caused to be carried out in amending and transferring MAs can be carried out by the EMA and national regulators, who will also be required to take up the activities that the MHRA has done as lead regulator for a disproportionately high level of authorisations.
In its evidence to the House of Commons Heath and Social Care Committee, Astra Zeneca noted that to supply its EEA customers from the UK as a third country, it would need to establish a new facility for batch testing and release which would take three years: “if a transition period is not agreed, and the UK us regarded as a third country from April 2019, then the supply of medicines to patients in the EEA could be disrupted.” Clearly if the UK were to reciprocate and treat EEA countries as third countries we could expect disruption to imports, which is why it is so important that the Government and the MHRA establish continuity of recognition for EEA products and operators – even on a unilateral basis.

The Fear and the Reality
What are the reasons behind the fears that supplies of medicines and medical devices will be at risk? Broadly they break down into three categories:
- Tariffs
- Regulatory barriers
- Logistical delays
1. Tariffs
Most finished medicines are tariff free under the EU’s Common External Tariff, while most developed countries keep medicines tariff free under a WTO Pharmaceutical Tariff Elimination Agreement. Yet there are some products like active pharmaceutical ingredients and intermediates that are not tariff free and would attract import duties. Most medical devices are also tariff free under the CET. It has been suggested that the UK should work in the WTO to update and extend the coverage of the Pharmaceuticals Agreement.
However, outside of the customs union, and with control over our external tariffs, the UK should unilaterally eliminate all tariffs on medicines and medical devices. Such tariffs are acknowledged to serve no protective purpose in domestic industry, and in this country are largely borne by the NHS. We cannot compel the EU to do the same, so if no free trade deal or transitional period is agreed they may need to apply tariffs to their imports of pharmaceutical products from the UK. While in some cases, depending on whether there is competition for the product, the manufacturer may absorb these, in other cases they will have to be ultimately borne by the EU consumer.
Elimination of tariffs would also avoid the administrative burden of applying for reliefs from duties where ingredients cross borders at different stages of manufacture. As it would take effect a “most favoured nation” basis on all imports from the EU and the rest of world this would also improve competition in the market and value for UK consumers.
2. Regulatory
Because of the sensitive and potentially risky nature of medicines and medical devices, they are subject to rigorous and comprehensive licensing regimes and regulation which is harmonised for the EEA. The EMA is the EU competent authority. The regulatory structure applies both to the products themselves, and to operators in the supply chain, from the holder of the marketing authorisation for the product (MAH) to the manufacturers, importers and distributors (who may all be the same person).
Product approval – marketing authorisation
There are different procedures available to achieve a marketing authorisation (MA). A House of Commons Library Briefing Paper summarises them as follows:
It is clear that the different routes mean there are gaps in single market, illustrated by the recent reports of northern European visitors to Spain suffering devastating side effects from taking a painkiller that is widely prescribed in Spain but not authorised on UK market. It is also notable that this has not caused border checks to be carried out between member states, despite such highly material differences – the supply chains are so highly regulated that border checks are not necessary.
Manufacturer/importer licence – MIA
Firms that wish to manufacture or import from a third country medicines that have a marketing authorisation require a licence known as an MIA. For manufacturers and importers in the UK that licence is issued by the MHRA. To qualify for a manufacturers’ licence the holder must comply with certain conditions, which include Good Manufacturing Practice (GMP), a set of principles set out in EU directives. Before issuing a licence permitting import from a third country, the MHRA will need to inspect the manufacturer’s premises in that country to ensure that it conforms to GMP. Each batch of medicine imported from duly authorised third country manufacturers must then be inspected and certified by the Qualified Person (QP) of the licensed importer, unless the manufacturer is in a country with which the EU has a mutual recognition agreement in place in respect of GMP. The EU has such agreements with Australia, Canada, Israel, Japan, New Zealand, Switzerland and the United States. Medicines manufactured in or imported to any EEA country can be distributed in any other EEA country where the marketing authorisation applies.
After Brexit, the UK and EEA members will be third countries to each other. This means that, unless arrangements are made, marketing authorisations issued by the MHRA will no longer be valid in the EEA, EEA importers will need importer licences be permitted to import products from UK manufacturers, and the EEA importers will need to carry out full batch testing on imported medicines from the UK (and vice versa).
Optimally, the EU and the UK will agree to continue to recognise MAs and MIAs issued by each others’ authorities, at least for as long as the UK elects to retain single market regulation in this field. It is intended that this will be the case if the withdrawal agreement is agreed, because the UK’s full participation in the single market will continue for the transitional period.
If the withdrawal agreement is not agreed, or if no final agreement on regulatory recognition is reached at the end of the transition period, fears have been raised that supplies of medicines will be at risk due to these regulatory barriers.
This would indeed be the case if neither side, took any action. While the European Commission and EMA’s notices and actions so far have been oriented at no deal preparedness (for example indicating that MAHs will need to make changes to their MAs, by transferring or varying them to be in the name of an EEA entity by the end of March 2019), it is clearly in the interests of both parties, and especially users of these essential products in the UK and the EU, to reach an agreement that will enable the lowest friction possible in trade in medicines.
If no agreement is reached, there are wide ranging actions available to the UK unilaterally to keep our market open to medicines from the EEA. For example, the MHRA could be empowered to unilaterally recognise MAs issued in the EEA under the central and decentralised procedures, and recognise GMP, GDP and QPs in EEA, to enable imports of medicines manufactured and licensed in the EEA, whilst continuing the MAs that firms already have in the UK. This would need to be conditional on EEA MAHs providing reporting and data to the MHRA that the MHRA would no longer be entitled to from EU databases.
The MHRA has stated that “if no transition period is agreed, we would ensure the minimum disruption and burden on companies as the UK exits the EU, while building on the existing relationship between MHRA and firms.” However its latest publication on 6 August 2018 addresses how the transition period would be implemented and does not provide any proposals on no deal planning. Given the publicity that stories of shortages and stockpiling are attracting, it would be beneficial for the MHRA to publish some information on the steps it can take to avert these scenarios.
Medical devices
Medical devices (which include everything from bandages and syringes to apps) are not subject to the same process of authorisation and licensing. They must meet applicable regulation on safety and be independently certified by a notified body. It is common in international trade to have mutual recognition of conformity assessment, but if this cannot be agreed with the EU the notified bodies must be EEA entities. To secure continued supply of medical devices from the EEA if no deal is agreed, the UK can continue to recognise EEA notified bodies unilaterally. For exports, most UK notified bodies are part of wider European groups, so can continue to certify medical devices for the EEA market as agents or sub-contractors and those that aren’t, like BSi have established a presence in Europe in order to be able to continue to certify products for that market.
3. Logistical delays
While the above unilateral steps would smooth the regulatory aspects, a key concern has been that pharmaceutical supplies will be caught up in delays at ports and airports. To avert this, pharmaceuticals companies and their intermediaries should be prioritised to become certified as Authorised Economic Operators (and for other trade facilitations that are available enabling goods to be cleared without inspection, and payment of duties and VTA to be deferred). Existing supply chain security from rigorous licensing requirements should mean that they will qualify straightforwardly.
The government should also seek recognition of the UK’s AEO scheme from the EU and other trade partners. However, the processes to streamline customs declarations and clearance that HMRC will need to put in place need to be clarified and publicised as a matter of urgency so manufacturers, distributors and their logistics suppliers can make the necessary arrangements. These should include postponed accounting for import VAT, and periodic self-assessment for customs declarations so that not every shipment will need to be declared.
For more details on unilateral facilitation measures that the UK government should be implementing see our briefing Under Control: What HMRC can do to prepare and optimise customs processes for all outcomes. The government is also working with manufacturers and distributors to ensure that sufficient stocks are available in the UK to cover supplies in the event of disruptions from a no deal scenario. The chief executive of the European Association of Euro-Pharmaceutical Companies (EAEPC) has said “excess warehousing provision is being sought by manufacturers in advance of next March so there’s sufficient supply already in place” but this can only be a short term, interim measure.
More strategic/long term concerns
Another important feature of the single market in medicines is the information sharing between regulators – “pharmacovigilance”. This enables data on medicines in the market (like adverse reactions) to be monitored and collated across a large population across all EEA member states. It would be highly beneficial to both sides for such information sharing and cooperation to continue, and there is precedent for this in the case of the agreements between the EMA and its counterpart in Switzerland. Even in the absence of international regulator information sharing, the UK could ensure that MAHs and importers continue to report to them on intelligence and developments from the market as condition for continued recognition of their authorisations.
Achieving MA for a medicine is a costly and time consuming process. The larger the market covered by an MA, the more viable it is to pursue. In the mid to long term this will be a key consideration for UK lawmakers, as there are clear benefits to maintaining alignment if full mutual recognition is available. Such benefits will need to be set against the gains that could be made from improving the regulatory system to encourage innovation and competition. If the UK were to continue to recognise EEA MAs, whilst also making improvements to our national system and working with regulators in other jurisdictions like China, Japan and Australia, to speed up authorisations, as suggested by Sir Michael Rawlins in his evidence to the HOC Health and Social Care Committee, this could mean the UK will benefit from more medicines being available more quickly.
Clinical trials regulation is acknowledged to be problematic, and the original EU clinical trial directive has been replaced by a new regulation, which will come fully into force in 2020.
The European Federation of Pharmaceutical Industries and Associations reports that 1,500 clinical trials are currently underway where the UK is the sponsor. While this does not affect the imminent concerns around supplies of medicines, the future of those trials, and the operation of clinical trials under the new regulation, which provides for trials to be regulated by a centralised portal, need to be resolved. Ultimately this is an area where the UK can play role in global fora, for example the OECD, which is calling on “member governments to harmonise their clinical trial approval processes. The aim is to encourage international collaboration in clinical research and streamline procedures for conducting clinical trials”.
Medicines and medical devices regulation is heavily influenced by international organisations like the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). The UK needs to apply for observer status in the ICH as soon as legally possible (ie the first day after we are no longer a member of the EU) in order to progress to full membership after two years under the rules of the organisation. Many people in the industry have suggested the UK having an independent voice in the ICH will be a benefit of Brexit.
For medical devices – participation in International Medical Device Regulators Forum – organisation of regulators from 9 countries (including Japan, the USA and China) and the EU working towards harmonisation and convergence in medical devices regulation.
In any event, investment in the UK by the pharmaceutical sector has remained strong, with Novo Nordisk, Astra Zeneca and GSK all proceeding with significant investments.
The European Perspective
It is becoming increasingly clear that the hard line taken by the European Commission and the EMA is in fact risking the supplies of medicines to the European market. The EMA has announced that due to its move from London to Amsterdam it expects to lose at least 30% of its staff. This, combined with losing the capacity of the MHRA, means that it will be scaling back activities. It is unclear how the additional work it has caused to be carried out in amending and transferring MAs can be carried out by the EMA and national regulators, who will also be required to take up the activities that the MHRA has done as lead regulator for a disproportionately high level of authorisations.
In its evidence to the House of Commons Heath and Social Care Committee, Astra Zeneca noted that to supply its EEA customers from the UK as a third country, it would need to establish a new facility for batch testing and release which would take three years: “if a transition period is not agreed, and the UK us regarded as a third country from April 2019, then the supply of medicines to patients in the EEA could be disrupted.” Clearly if the UK were to reciprocate and treat EEA countries as third countries we could expect disruption to imports, which is why it is so important that the Government and the MHRA establish continuity of recognition for EEA products and operators – even on a unilateral basis.

3 thoughts on “Brexit and pharmaceuticals – separating fear from reality”
Comments are closed.
SHARE



“If the UK were to continue to recognise EEA MAs, whilst also making improvements to our national system and working with regulators in other jurisdictions like China, Japan and Australia, to speed up authorisations, as suggested by Sir Michael Rawlins in his evidence to the HOC Health and Social Care Committee, this could mean the UK will benefit from more medicines being available more quickly”
So the UK would rely on other countries to make the decisions over what drugs are licensed, without any input into the regulatory system?
That is what I call TAKING BACK CONTROL. Oh no… Wait…..
Marc, I’m not correlating co-op with other states meaning a loss of control. In fact the central tenet of the document is how, having control, we could unilaterally completely eliminate tariffs on this sector, given it has apparently limited impact on industry protection.
By the way, writing in capitals doesn’t strengthen your argument.
Manufacture in the UK.
Simple really.
Just seen a minor wound spray by Elastoplast made in Germany. Come on, surely we can do better than this.
Chris